Frozen shoulder and rotator cuff injuries and degenerative rotator cuff issues are the main shoulder diagnoses that come to see me. But add to that a myriad of stiff shoulders, tight necks, sore mid-backs, pain when lifting the arms and whiplash spreading from the neck down to the shoulder blades and then the number of clients I see with shoulder issues is over 70 percent. If I then add the number of people with stiff mid-thoracic spines and compromised rotation, then I could look to the lack of efficient movement of the shoulder blades as a possible cause, which then takes that figure up again.
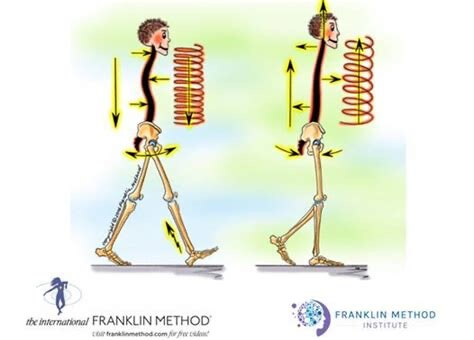
And lets not forget stiff hips – immobility and tension at the shoulder joint, will inevitably affect the hips in walking as if you can’t swing your arms easily the counter movement at the opposite hip is affected – i.e. your stride length will be shortened.At this point I could argue that happy shoulders means a happy rest of the body! Personally I believe that argument could be justified for any body part. Happy feet means happy rest of body, happy ribcage means happy rest of body, happy hips means happy shoulders etc. But I digress…. So what to do about those shoulders?
The shoulder blades are typically taught as moving in 6 directions – elevation (up) depression (down) upward rotation, downward rotation and protraction (forward movement) and retraction (backward movement). This break down of the movements into their component directional parts is true, but also not true… in that when we actually move we move through all planes of movement and in multiple directions simultaneously. So splitting this all down into a way we can give our clients an experience of efficient movement is super hard – especially when it may be unclear where the root of the problem is.
My solution? Use Eric Franklin’s concept of the shoulder blade muscles as a team. You want the team to work together, however you need to check the health of each player individually otherwise the whole team can’t function. It would be like playing football without a goalie…
I like to start with the trapezius muscle – 9 times out of 10 this little star player thinks it can do all the work – its trying to play solo and then running out of steam. First things first lets give this one a breather. Use massage, muscle sliding imagery, touch, sponging imagery or focus that when you drop your arm from a lifted position, the upper trapezius has to lengthen again. Use pilates or yoga to get the muscle lengthening and shortening – your choice.
Next – levator scapulae. As this little one attaches from your neck to the inner upmost corner of the shoulder blade when your arm lifts, as the shoulder blade spins, this corner goes down so this one lengthens. Is yours? Or like many players on a team is it stuck only doing one half of its job that it now prefers (elevating the shoulder blade)!
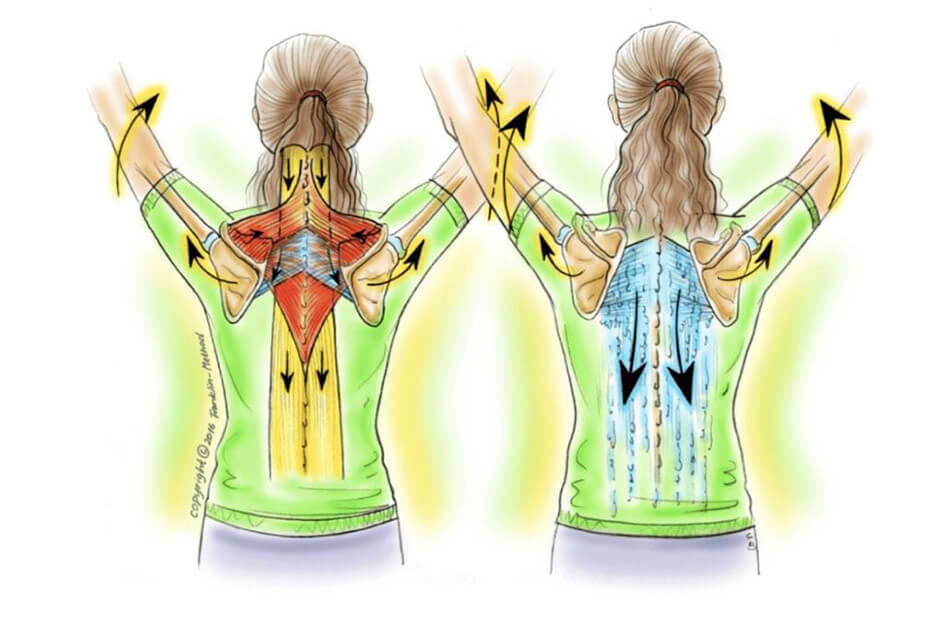
I’m not going to go through every team member here, but there are lots to check out. Rhomboids, serratus anterior (upper and lower fibres do different jobs at different times) mid and lower trapezius, then all the rotator cuff muscles and deltoids and lats….phew! It takes time and patience to work through them all, but the benefits can be extraordinary. If they all work well together then as you raise your arm your shoulder blade spins as it is designed to do, meaning the humerus or arm bone has support underneath it, and the rotator cuff muscles get the assistance they need.
So often, when I inherit a client from someone else for a shoulder injury (particularly a rotator cuff injury, the focus has only been on that particular rotator cuff muscle and maybe others in its immediate group. And often the patient is asked to focus on one muscle for several weeks (or until the next appointment). But if you think about it for a moment that makes no sense. The rotator cuff muscles fix the humerus into the socket of the shoulder blade (glenoid fossa) but the glenoid fossa, as it is part of the shoulder blade itself, can move all over the place – it doesn’t stay still. So when you lift your arm, you need to make sure the socket is moving in a direction that doesn’t put extra strain across that joint which in turn means extra strain on those rotator cuff muscles. By which I mean you need to train the 3D movements of the shoulder blades too.
Thinking about the individual team players is important, but sometimes the fastest way to change is by imagining what you really want. Focus on the right image, which holds within it the missing component that you are not doing and that is often the fastest way to create change, as done well, it can instantly remove unwanted tension from an area.
Suddenly the client is able to move both arm and shoulder blade, whilst still ensuring the one muscle they were asked to focus on is doing its job. Imagery allows them to put that muscle back into context.
Timing is everything. And timing as all good football teams know only works when a team pulls together!